The Twenty Truths of Direct Primary Care
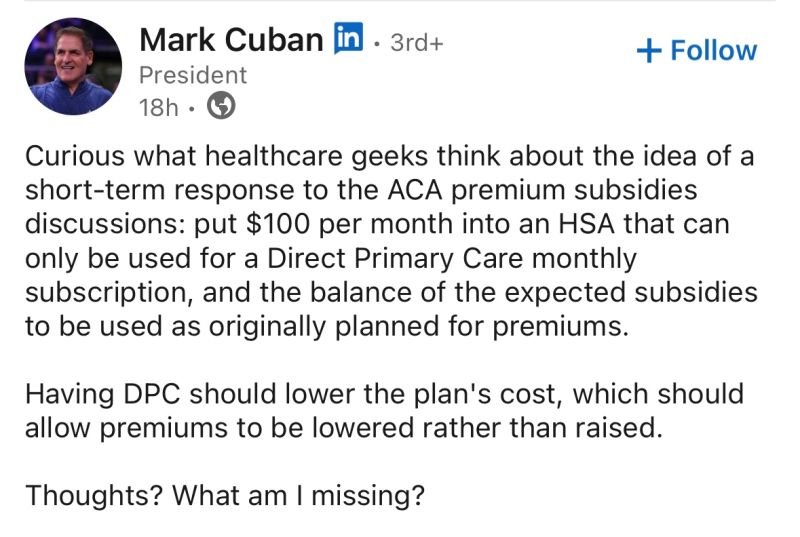
Mark Cuban has been active in the DPC and cash pay space recently. I wrote these 20 truths of DPC on LinkedIn to give him a quick rundown. These are points I think anyone new to DPC should know and are based on a decade worth of experience in the space.
1. Primary care is prevention and maintenance. Insurance is coverage for catastrophes. This is why direct primary care makes sense.
2. DPC works best when it goes direct to consumer. https://dpcnews.com/opinion/dtc-the-key-to-dpc/
3. Some patients value access when needed, others like the predictable cost for frequent utilization. Most of the reasons can’t be captured by the usual “quality” measures.
4. There is only so much primary care patients can consume. No one abuses the unlimited visits DPC offers.
5. DPC is inherently different from any other insurance based capitation arrangement. https://dpcnews.com/resident-and-student-section/dpc-vs-capitation/
6. DPC does not bear risk in any way or form.
7. Hospital systems can’t do DPC as it goes against their fundamental business model.
8. “Value based care” is an admin heavy, insurance based game. DPC is the opposite of that.
9. DPC does not equal concierge. They are different in payment model and core philosophies.
10. Employers have grown the DPC movement but anything without a direct to consumer aspect is just an onsite/near site clinic and not DPC.
11. Membership fees are currently much higher than traditional spending on primary care. This is a good thing.
12. There are two different core types of DPC- individual mom and pops and larger groups (usually at least 3 locations with more than 5 doctors).
13. Individual practices are highly varied in offerings and pricing. They generally won’t track or provide any population level data.
14. Larger DPCs tend to work with employers and have more data collection, including ROI measures, and standardization.
15. A lot of the current success of DPC comes from the current group of DPC doctors who are mission driven, hard headed, and talented enough to buck the system and succeed. Fighting the system may be a prerequisite to getting the right people to do DPC.
16. The model has been around for almost 3 decades, but the rapid growth has been only within the last 5-10 years.
17. There’s generally not enough margin to justify much administrative overhead which is largely considered a good thing in the DPC community.
18. Exceptional care navigation/patient advocacy is inherent in the model and perhaps its most underrated aspect.
19. DPC is not a panacea and should not be expected to solve all the woes of the current system. It is however the only thing radically different enough to create meaningful change. https://dpcnews.com/dpc-motivational-tip-of-the-day/best-of-dpc-news-side-effects-may-include/
20. DPC, as it exists today, has room to develop and evolve. https://www.youtube.com/watch?v=NhoVfg6Ueo4






As usual for Kenneth, concise, insightful and right on the money. I hope Mark Cuban is listening and adjusting.
Should #11 read “membership fees are lower” (not higher)?
Thanks for this, really nicely broken out. I think these individual points would make some great social media posts!