Do Hospitals Want Patients to Be Healthy?
I remember when I was in the system and received a group email from the CEO. He was concerned and warned us that admissions were down. My head almost exploded. Wasn’t my goal to keep patients out of the hospital? This is the problem with doctors being employed by the system. There are so many conflicts of interest that it makes you go crazy. In that situation, I asked the CEO if he wanted us to create more sick people and put them in the hospital. I was known to them as a problem child. He said no and wormed his way out of it with some Administralian talk. But we all knew what he meant and what he wanted.
Recently, Forbes put out this article called When Patients Win, Hospitals Lose and it’s de ja vu all over again:
A senior healthcare administrator recently shared a story that should unsettle anyone who believes our health system exists to promote health.
He was called into an “emergency summit.”
Not because quality was declining.
Not because outcomes were worsening.
Not because access was deteriorating.
The crisis was this: heart failure admissions were falling.
The cardiology team had dramatically improved outpatient management — tighter follow-up, optimized medications, early intervention. Fewer patients were decompensating. Fewer were landing in emergency departments or ICUs.
Patients were healthier.
So the meeting agenda became: How do we increase heart failure admissions?
Read the rest of the article, as the author does a good job. He claims the arguments for this issue are:
- Argument #1: “Our costs are fixed. When volume drops, we collapse.”
- Argument #2: “Value-based care doesn’t replace lost revenue.”
- Argument #3: “We have to protect profitable service lines to fund everything else.”
- Argument #4: “If we don’t keep volume, someone else will.”
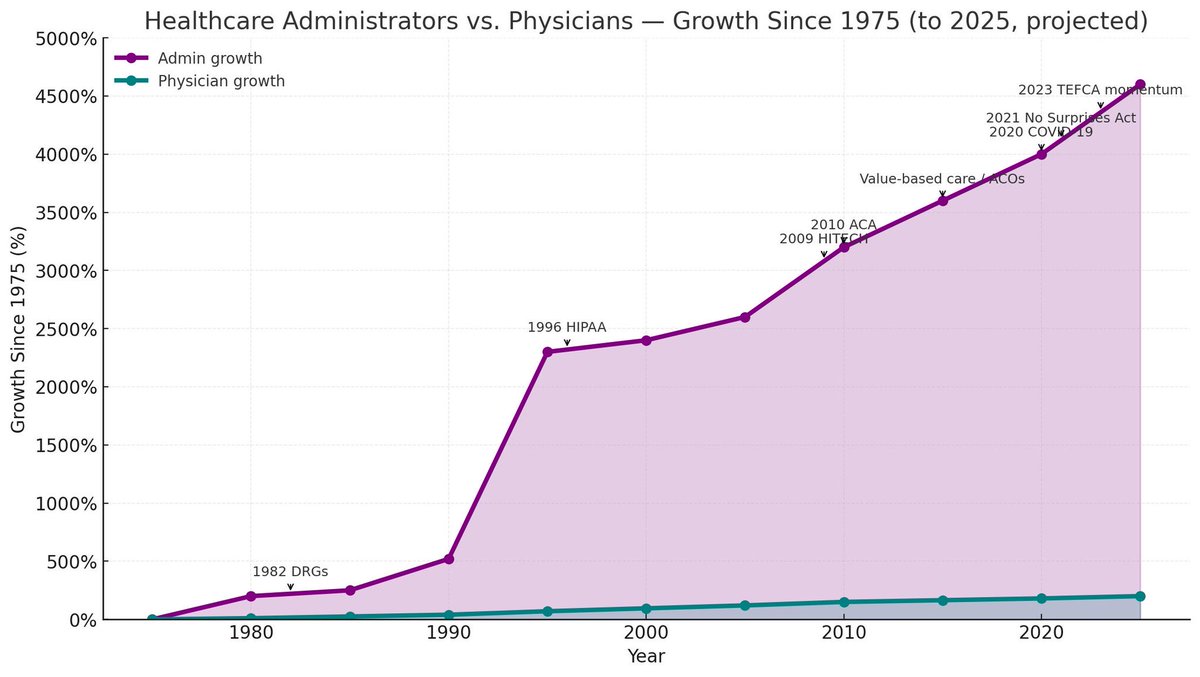
He goes into detail on each of these, but what he conspicuously fails to mention is the bloat of administrators that drain the system.
Why would he ignore this?
Could it be that Sachin H. Jain has “worked in clinical medicine, academia, government, big pharma, and the health insurance industry. I am President and CEO of SCAN Group and Health Plan, a $5.5B non-profit entity that serves over 350,000 patients. I have worked in leadership roles at Merck and Company and the US Department of Health and Human Services, and have held faculty appointments at Harvard Medical School and Harvard Business School?”
Yes, he is a career administrator.
Listen, I give him credit for calling out the same situation that I had years ago, but to not mention the explosive growth and waste of administrators is ridiculous.
Here is what needs to happen. Physicians need to break the shackles of hospital employment altogether, as it is a conflict of interest! That is what bothered me the most in my story above. This article wouldn’t have happened if the doctors were independent.
Direct Primary Care has shown ALL physicians how to do this.
- Stop billing insurance.
- Stop being employed by big hospital systems.
How did hospital systems survive in the old days before they bought up every physician’s office? Let them follow that blueprint. They won’t because they would have to fire 90% of all administrators. It doesn’t matter because they need to figure that out in the future.
The only way this healthcare system gets fixed is with physicians doing the trailblazing. Direct Primary Care and Direct Specialty Care are the way. Our goals are aligned because we want to keep patients healthy. The rest can follow or risk failing.





The real problem is in how reimbursements happen. If big systems are going to work (which would probably only happen with a single payer system), then systems need to get paid for keeping people healthy, not for ICU admissions. I waited 25 years for the system to change, and I finally stopped waiting and switched to DPC. If enough primary care doctors do this, it will FORCE the system to change. Not holding my breath for it to happen before I’m long gone from clinical practice.