DPC-Centric Health Plan Architecture and Construction – it’s a lot like building a house.

If you follow me on social media, you’ve seen me use this graphic repeatedly. It portrays the “vertical integration” of the BUCAs (Blue Cross, United Healthcare, Cigna, Aetna). As a matter of fact, I suspect that “medical trend” (an ever-increasing factor used in pricing health plan premiums) is a made-up number used to help fund the future acquisitions for vertical integrations. In other words, employers are funding the growth of the BUCA empire. Stated another way, the BUCA empires are rapidly growing almost solely funded by employers and employees.

Figure 1: Credit to Adam Fein of Drug Channels Institute
In most other corporations, vertical integration isn’t a bad thing. For instance, keeping with the architecture and construction theme, if a home builder wholly owned a paving company, no one would bat an eye. Most folks would just realize that the vertically integrated company services the home builder by paving driveways, pouring concrete for patios, etc. Conversely, when the companies listed in the graphic above acquire or merge with other healthcare services the intent is more or less to hide money.
The most egregious example of this behavior is when these companies added PBMs (pharmacy benefits managers) to their vertical stack. This move was intentional, especially after the Affordable Care Act was passed and incentivized these companies to hide as much money as they could. The more money they removed from being considered revenue, that would have to be reported and considered part of the MLR (medical loss ratio), the better. Better for them…not anyone else.
Lots of stories have come out in the last few years decrying how PBMs drive prescription drug costs higher. Many of us here on the ground have been sharing the same message. Well, the Federal Trade Commission finally agrees. Today’s news brings this headline to the forefront — Big Pharmacy-Benefit Managers Increase Drug Costs, FTC Says (msn.com).
Here’s the good news for DPC. You can dispense some of the same drugs, sans the PBM, and save money your patients, the employers in your area, etc. This is something the employers in your area really need to know.
The Consolidated Appropriations Act of 2021 requires employers, PBMs and the carriers they associate with to reveal paid prescription drug claims every year. It’s called the RxDC reporting. It’s due every year by June. This data is consumed and is supposed to be publicly available.
Here’s a call to action for you. Request last year’s RxDC report from your local county government. Offer to analyze the report (I can help you with this) and return information back to them about how much lower their plan can purchase the drugs in the report through your DPC pricing methods (which doesn’t include the PBM price hikes). It’s a great place to start a conversation about the untapped value you bring to the table.
Why did I recommend your local county? Because you have a vested interest in helping them reduce their costs. You are paying taxes to them after all. That means you deserve answers about how your tax dollars are spent. Plain and simple. Maybe you don’t lead with that line of thinking, but maybe you just offer to lend a helping hand and hope it leads to a new client relationship.
Lastly, you may have struggled to explain how a properly constructed health plan functions. When DPC is at the foundation of the plan, it looks a bit like the graphic below. Like a house built on a firm foundation. That’s how health plans should be. The DPC foundation firms up the way the rest of the plan is built. The other “bricks” in the house can be other local, independent, healthcare partners. This is especially important when constructing “community-owned health plans”. I’m sure I’ll write about that someday soon.
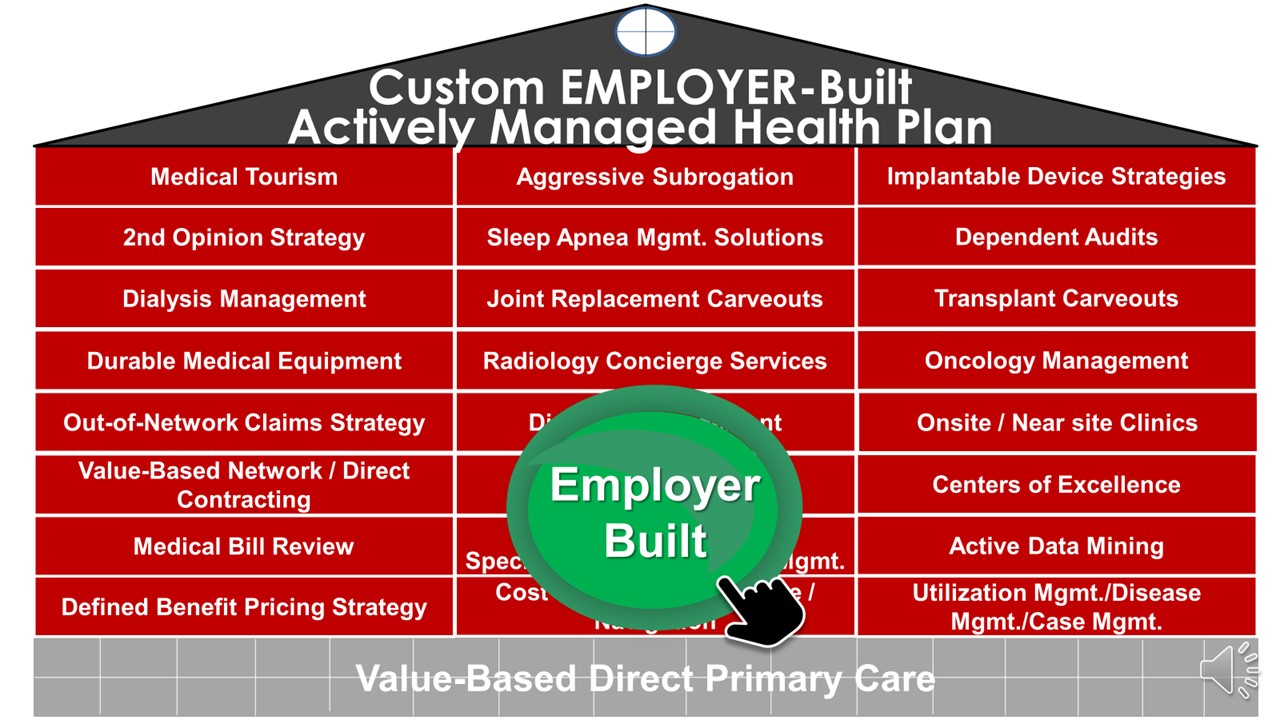
Figure 2: “Employer-built healthcare vs. Insurer-built healthcare” credit — Mitigate Partners
Well, that’s probably enough for now. I’ll check in with you again soon. I want to thank DPC News for allowing me this platform to share my knowledge and passion for seeing employers work directly with independent, physician-owned, local DPCs.






Great info. Good to have you on the team.