Authorizations — Part 1

Before we get started, let’s revisit prior authorizations with Dr. Glaucomflecken in this video — How to Get an MRI – YouTube. It’s always fun to laugh before we must talk about such a frustrating topic.
Ok, now that we’ve had a chuckle…I’ve been thinking about prior authorizations lately because my state’s legislature recently took up the subject matter and is trying to insert themselves into it. The problems PAs cause your patients aren’t going to be solved in this article nor are they going to be solved by anything other than a change in the way your patients pay for their care.
Obviously, by way of them becoming your patients in the first place, they’ve at least changed the way they pay for primary care. However, if care is needed outside of your DPC practice, it could mean interacting with the PA beast, but only if certain “processors” are in the mix.
I use the word “processors” on purpose. Many use the term “payers” to describe third parties who “pay” claims. Let’s not dance around this. The BUCAs (Blue Cross, United Healthcare, Cigna and Aetna) don’t “pay” for anything. They just move other people’s money around in ways that profit themselves. Copying fellow Mitigate Partner, Carl Schuessler, I’ve adopted the term “processors” because they process claims. The only true payers in healthcare are employers, employees, individual patients, and taxpayers.
So, the processors want patients to take extra steps before they agree to approve a claim. I believe today there’s less of a chance that they’re actually looking to find the best option for delivering this care. I believe they’re merely trying to redirect the care to the nearest vertically integrated option. Because the BUCAs now own more of the healthcare supply chain than ever before, they have a vested interest in slowing down the claims process to ensure their vertically integrated, wholly owned entities are delivering the care they then process the claim for.
Recently, I read one of the best descriptions of the vertically integrated supply chain managed through Aetna – CVS/Caremark – CVS Pharmacy processing machine. Dr. Seth Glickman is a guest writer on Wendell Potter’s Substack newsletter Health CARE Uncovered and he wrote “Gaming the System: Medical Loss Ratios and How Insurers Manipulate Them”. It is definitely worth a read.
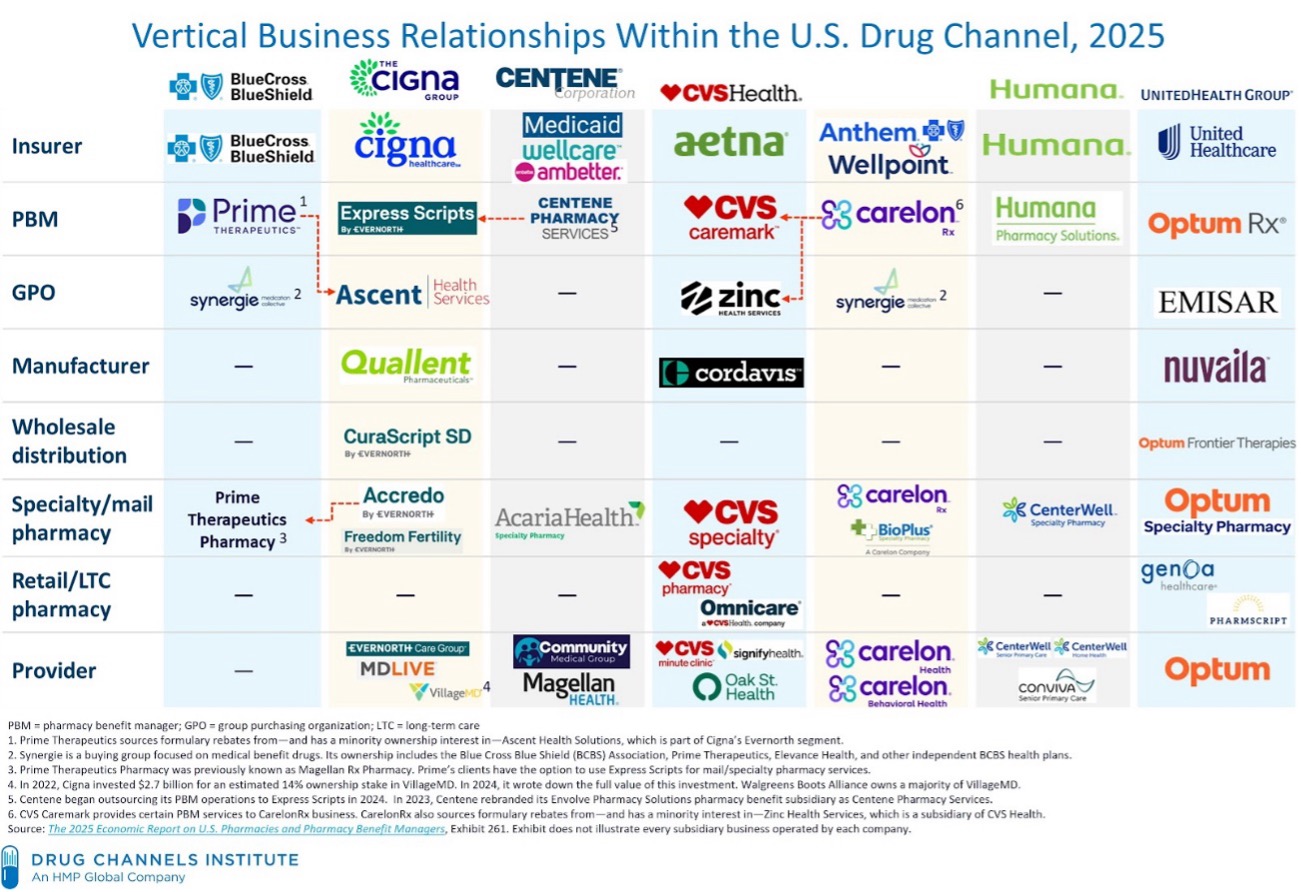
In the above picture published by Adam Fein of Drug Channels Institute, it carefully outlines the vertical integration that Dr. Glickman exposed in his article. However, vertical integration doesn’t stop there. In my state of NC, our insurance commissioner, Chris Deacon and myself gave a valiant effort to warn North Carolinians of the future acquisitions BCBSNC was about to undertake if they didn’t reconsider a bill allowing them to pivot back and forth between for-profit and non-profit when it pleased them; escaping transparency and oversight. We recorded this podcast about it — S3E04 – NC H346s Hidden Motives with Christin Deacon and Mike Causey | Custom Benefits Solutions. BCBSNC needn’t worry, their strategic planning to get the NC lawmakers to agree to pass the bill before it was ever filed worked. Only a handful of legislators voted against the measure, and it became law.
Guess what happened next? Yep, they acquired the Fast Med Urgent Care Centers in NC and the newly vertically integrated entity was all set. I don’t have any hardcore proof of this, but I certainly believe this setup gives them the ability to practice “gold carding” (mentioned in the podcast above) where when BCBSNC processes a claim it sails through (no PAs needed) at a much higher price than normal and nobody says a thing. And how could they say anything? It’s practically untraceable in the data. The folks who pay premiums on the policy presented for payment won’t see the results of this processing manipulation until it’s time to renew that policy that year or sometime in the future. The double-digit renewal increase will force the real payer to water down their policy, accepting more and more cost shifting just to keep carrying around that ID card in their wallet.
I might not write about PAs being the redirection to higher priced care if I hadn’t experienced it for myself. I’ll tell you that story next month.





