Health Insurance Has Not Aged Well

Written by Liz Fischer
Robert McMillan Aged Well, Health Insurance Did Not
“BCBS of Texas began in 1928 when a former Dallas school superintendent took on a role with Baylor University and was in charge of the Dallas hospital units. He created a plan allowing teachers to contribute to a fund guaranteeing them up to 21 days of hospital care at Baylor in Dallas. The “Baylor Plan” was the original commercial plan, and future leaders began considering community-wide plans to fund members’ healthcare.” Source: D Magazine
If you are contemplating converting an existing insurance-based practice to DPC you may have a patient like ours who, when he is run through the mill of your industrial practice, makes you keenly aware of how terrible that experience has become for both the doctor and the patient. My husband longed to have more time with Mr. McMillan, in part because he was delightfully formal and incredibly interesting – the kind of person who makes you wish that you weren’t in a rush. We desired to create a clinic where Ben could interact with this beloved patient in an unrushed human-paced manner and to care for him how he might have been cared for in the first half of his life, before the intrusions of third-party payers. Our patient was born in 1923, a fact that led me down a rabbit hole trying to get an idea of what American medical care was like when he was born. What I found out was that our patient was about the same age as The Baylor Plan which became Blue Cross/Blue Shield of Texas. Health insurance changed dramatically over Mr. McMillan’s lifetime. The following is a back of the napkin sort of analysis that I sometimes do when I probably should be doing something more productive.
Fischer Clinic opened 100 months ago. I realized that when I archived one of our founding members, Robert McMillan, who died last week at the age of 100 and I noted that he had made 100 monthly payments. Mr. McMillan was the person who gave my husband, Dr. Ben Fischer, and me the strongest desire and urgency to start a direct primary care practice. Our family attended his 90th birthday in 2014 where he held court telling stories in his beautiful yard that he had probably mowed himself–always in a necktie and signature straw fedora hat. At that time, there were only about 200 DPC practices nationwide, and we were eagerly learning what we could, impelled in part by the desire to open while Mr. McMillan was still alive. We had no idea we would enjoy caring for him for another 10 years!
In 1928, the Dallas school superintendent who started working at Baylor University presumably wanted to make hospitalizations more affordable to teachers – which sounds like a good idea especially if, as one would assume, teachers could not otherwise afford hospital bills. The pre-paid plan called the Baylor Plan worked roughly like this, Teachers paid 50 cents per month (equivalent of $9.18/month in today’s dollars) for up to 21 days in the hospital. What that means is a teacher in 1928 would pay $6 annually ($110.16 in today’s dollars adjusted for inflation) for up to 21 days in the hospital. That made me wonder a few things. 1. How much did a hospital stay cost in 1928? and 2. How long was it before they had to make changes in the Baylor Plan?
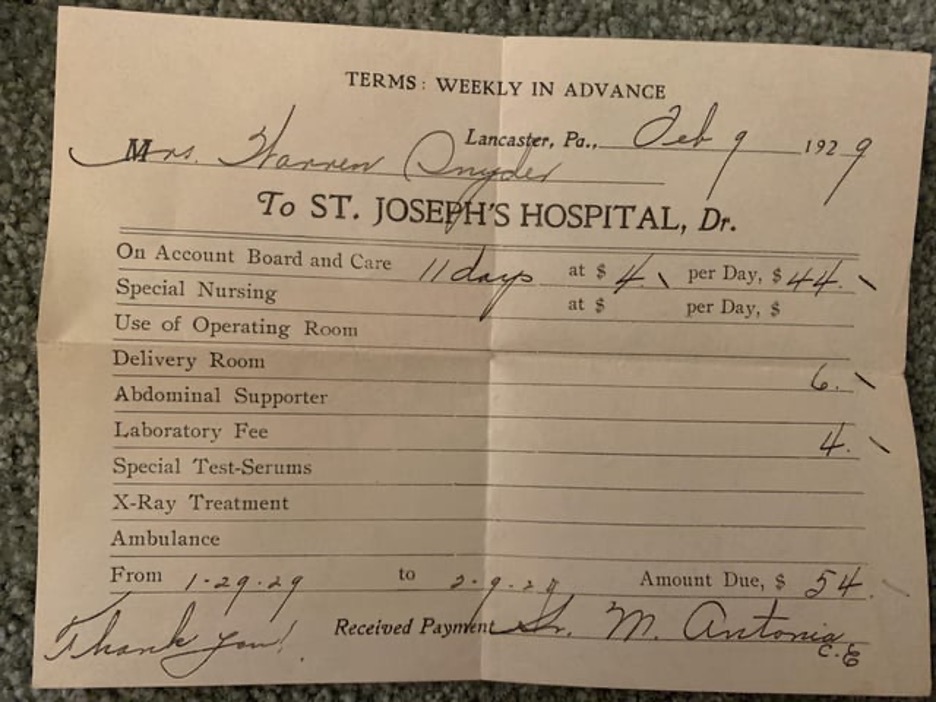
For reference on in-patient hospital pricing, I found a $54 hospital bill from 1929 for a birth which included an 11-night stay. The per day “Board and Care” rate was $4/day with itemizations of $6 “Delivery Room” and $4 “Laboratory Fee”. In today’s dollars that would be $992.13 for childbirth including an 11-night hospital stay.
Today, there is no way to compare apples to apples but there is certainly no plan that would guarantee up to 21 nights in the hospital for $110.16 annually. If the cost of hospitalization were the same today as the childbirth bill from 1929 above, then that stay in today’s dollars would cost $92 per night or $992.18 for 11 nights. Anyone who has received an itemized hospital bill can attest to the fact that $92 might not even pay for one aspirin. Today, the national average nightly stay at a public hospital is $3025, so an 11 night stay now would cost approximately $33,275.
Although employer-based insurance plans today include “coverage” for both hospitalization and other medical care, there is no offering that even remotely approximates the value of that original plan. The average monthly cost of an employee plan today is $686.75 per month for the employee alone and doesn’t include the cost of the deductible (probably high) and co-insurance. It DOES include rationing though networks, denials, surprise bills and prior authorizations. The average price of health insurance premiums for single coverage is now 84 times higher than the original Baylor Plan (with coverage less certain) and the average price of hospitalization is 33 times higher than in 1928.
Cost of Baylor Plan compared to Average Employee Plan Today
| Baylor Plan (in 1928 dollars) | Baylor Plan (in Today’s Dollars) | Average employee only plan today | Price today compared to 1929 | |
| Insurance Premium | $0.50 monthly$6.00 annually | $9.18 monthly$100.16 annually | $703 monthly$8435 annually (plus copays, and co-insurance and cost of whatever is care is denied) | 84 times higher |
| Coverage | 21 days in the hospital | Less and less – certainly not 21 days in the hospital with no deductible or co-insurance |
Cost of Hospital Stay in 1929 compared to 2022
| 11 Days in the Hospital | In1929 | 1929 bill in today’s dollars | 2022 | Price today compared to 1929 |
| $54 actual bill from 1929 | $992.18 ($54 adjusted for inflation) | $33,275 (avg. $3025 per day) | 33 times higher after adjustment for inflation |
While the Baylor plan started in the 1920’s with a beneficent mission at modest expense, it spawned the malignant growth of a health insurance industry that has grown into a profit seeking monster with far too much power over patients and physicians. This power has imparted a level of control to the health insurance industry that is primarily responsible for the dramatic inflation of health care costs and decline of health care quality—especially if you are measuring quality from the perspective of the patient. In the meantime, our patient, born in 1923, became wiser and more interesting and charming with every passing year. If only Blue Cross could have grown up the way Robert McMillan did—leaning from his experiences—both successes and failures– and focused with humility on doing justice, and faithfully serving his clients.
Mr. McMillan was born with a good mind and heart and was raised on the right principles that started him on a trajectory to become the good man he became. Blue Cross, while seemingly well-intentioned at the outset, was founded on tragically inappropriate principles that set it on a course to grow up to be the greedy, tyrannical entity insurance companies have become. The basic idea that is wrong with all third party paid healthcare is that doctors, nurses, and hospitals no longer work for patients; their accountability is perversely shifted to the payer. That basic error in the founding DNA of Blue Cross set the stage for the disaster we have today. Now, instead of independent doctors caring for individual patients within hospitals, we have employed physicians and nurses working within a corporate industry. This industrial model, blindly serving the bottom line of shareholder equity, can be profligate in its billing and spending due to collusion between insurers, hospitals, big pharma and other “middle man” players, all of whom benefit from skyrocketing costs. Meanwhile, the patients suffer, and the doctors and other providers pay with their souls, having lost almost all control over what should be the modest and distinctly human endeavor of people caring for people.
If only we could go back to 1928 and put the genie back in the bottle, telling the presumably nice man with the noble intention of making health care more affordable for teachers that what he started with good intent was fundamentally flawed and destined to become a force for ill in the world. While we cannot do that, we can make the relationship between primary care doctors and our patients right again. One at a time, we can care well for beloved patients in a direct way that allows doctors and patients to experience the joy of creating and nurturing a fully authentic, therapeutic, and mutually rewarding relationships with each other. As a side note, Baylor and Blue Cross nearly broke up this year when they couldn’t come to an agreement on reimbursement terms. “Baylor Scott & White Health to Terminate Blue Cross Blue Shield Agreements in July”





