Empathy Through a Blurry Glimpse of Medical Anxiety

Witness the Birth of Lassey’s Scotoma Paradox
When I was a 3rd-year medical student on my pediatrics rotation, our attending physician had the students enter a room and take a seat around a big table. In walked a fully-prepared pharmacist, carrying a tray full of small plastic cups. Each cup contained an ounce or two of commonly prescribed pediatric drugs. The drugs were passed around and we each were asked to sample a couple of mLs of each drug. “Empathy for our pediatric patients,” the attending said, “must be gained through experience. Try the liquid prednisone. If you can’t keep that disgusting stuff down, how do you expect a 5-year-old to?” He was right, that stuff was nasty and all the sugar in the world couldn’t cover up the flavor of rotten eggs. When we can empathize with our patients, usually we’re better at our job.
We primary care docs see anxiety every day. I once read a reference to a study that claimed that 77% of visits to family physicians are either caused, or exacerbated by anxiety. I believe that, and I wouldn’t be surprised if it’s higher.
I’ve always been grateful that I don’t suffer from anxiety, as I’ve seen it cause so much debility to patients. I teach patients about resilience and optimism and coping strategies, and do my best to treat the problem. I frequently share a 5 minute online video that I love with my anxious patients. The video features UCLA Medical School psychiatrist Dr. Stephen Marmer teaching about resilience to common stressors, and I suppose having watched it a hundred times with patients has been therapeutic for me too.
But this last week I got my first glance at what it’s like to have uncertainty in your medical situation and much like that liquid prednisone I gagged down 23 years ago, I got a bitter taste of the anxiety that medical uncertainty provokes.
I’m quite far-sighted, and as my eyes have gotten older (note my stubborn refusal to admit the rest of me has followed suit) it’s just gotten silly with the myriad of lenses I have to look through, especially for certain procedures. So at the advice of my fantastic optometrist who is one of my DPC patients, I decided to pull the trigger on eye surgery. Replacement lens implants: permanent long-term vision correction with the added bonus of no cataracts in the future.
The current state of the art is Light Adjustable Lenses. Basically like cataract surgery lens replacements but a month after the eyes heal from surgery, they can use focused intense UV light beams to change the lens shape and really dial your vision in. Crazy sci-fi robot eye tech, we’ve got in this brave new world.
So I had the procedures, a week apart. Things went well. I was told to wear doofy UV-blocking glasses for a month with my somewhat blurry vision, while waiting for my eyes to heal for my light adjustment treatments. I was really pumped to get my eyes fixed and was about a week from my first treatment when I began to question if I made the right decision to get crazy robot eyes.
My treatments had to be delayed a week while I used PRP to cure some corneal dryness that was a complication of the surgery. I made my own PRP and got my corneas all healed up. No worries, I thought, just a one week delay. But then one day before my rescheduled initial light treatments, I awoke with left central scotoma. For our non-physician readers, as you know, we doctors like to use fancy-schmancy words for everything to make ourselves sound smarter than we really are. In this case, left central scotoma is the fancy word for loss or partial loss of central vision in the left eye. Where my left eye focuses, I have just a blurry gray circle.
My eye surgeon is an hour away, and I had a full clinic that day. But I was able to slip out and run to my optometrist’s office nearby. Her partner was covering for her on her day off, who took a look with the slit lamp and told me I’d developed scarring in the posterior capsule and that my eye doctor could treat it with the YAG laser. I felt better.
The next day, I went to the surgeon’s office. Told her about the scotoma, and she looked with the slit lamp and said that yes I had a little posterior capsule clouding that might need treatment eventually, but it wouldn’t cause my scotoma. I could tell she was worried that something else was amiss. She scanned my retina with a fancy German machine that probably cost more than my whole clinic, and that triggers something self-employed people call “overhead-cost-PTSD-flashbacks,” and with this fancy machine, she found this:
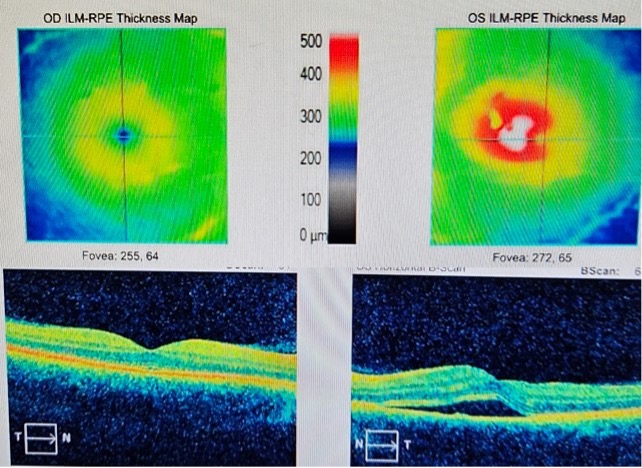
The picture on the lower left is a cross section of my right retina, and is normal. The little dimple seen in that picture is the fovea- this is where your central vision is focused and where the highest resolution vision is located in your eye. Note the differences from that side to the other. The fovea should be around 250μm (micrometers) thick. My foveal thickness is too thick (409 μm) due to fluid under the fovea, with layers of my retina getting spread apart with fluid much like an air bubble under a cell phone screen protector, a bubble under wallpaper, or a weasel in-between your bedsheets–you get the idea.
My eye surgeon felt that I had developed a kind of swelling called macular edema. Older patients with health problems, with whom she has more experience, sometimes develop a problem called Irvine Gass syndrome after cataract surgery. It’s a kind of macular edema that is at least similar to my issue, and is successfully treated with steroid drops.
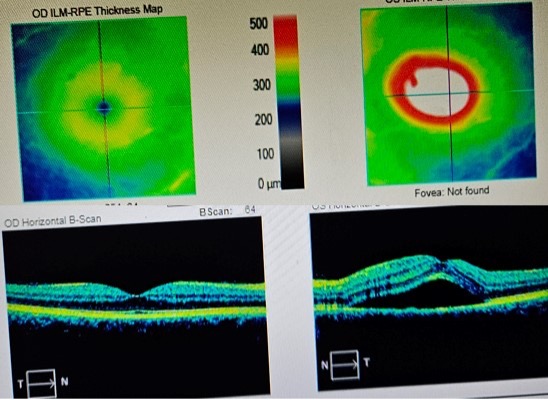
So she put me on steroids, confident that it would improve. But it didn’t and actually continued to get worse. After 6 days, my optometrist, who also owns a fancy German eye scanner/overhead PTSD machine, wanted to map my retina again, and my foveal thickness had increased to 587, my left eye vision now having become severely impaired. Here’s the scan. You know it’s bad when it says “Fovea: Not Found”:
That was when I got a taste of medical anxiety. My optometrist kinda freaked out and wanted me to see a retina specialist immediately, which is a tall order, the nearest one being a couple hours away and booked out for months. There were a few hours where I really had no idea what was happening to my eye, which seemed to be tearing itself apart for no good reason. I had no idea if my left eye would ever see properly again.
I have no diagnosis. My optometrist has no diagnosis. My eye surgeon isn’t sure what’s going on and has done thousands of these procedures and has never seen this. Uncertainty began to shake my generally-solid mental foundation. What if this? What if that? I do lots of procedures–can I do them safely with one eye? All the resilience training helped me to do a pretty good job of reminding myself to remain gracious- I was thankful for the other eye working, the many years of good vision I was blessed with up til that point, etc. Perhaps I could cash out like a bandit on my disability insurance policy and ride one-eyed into the sunset like Snake Plissken. I can find a silver lining to any cloud. But I was still scared.

It was during this time I was extremely blessed to be a DPC doc with close DPC doc friends. I shared my anxiety with a few close friends who I knew would send up a prayer for me. And they did. And they also had retina specialists on speed dial they were ready to call for me at a moment’s notice. I felt loved.
Our prayers were answered a few hours later, when good news started coming in: My eye surgeon had finally gotten in touch with a couple of retina specialists, who looked at the scans and confirmed that the diagnosis was not any form of macular edema, but rather Central Serous Choroidopathy, which is a rare complication of surgery that is exacerbated by the use of steroids after surgery, as well as testosterone and stress hormones, and my wife assures me I have too much of both. Then more good news: stop steroid drops and in 8-12 weeks, the condition should fully resolve. PHEW!
I was overcome with gratitude not only for the proper diagnosis but of course the good news that I can expect full resolution of these symptoms. Also with gratitude for friends and colleagues who I knew would be my shoulder to cry on. After a bit of reflection on this, I was also gracious for the opportunity to have experienced this anxiety (and very thankful that it was so brief!). I can only be a better physician having experienced this kind of uncertainty. My patients often have similar feelings when awaiting scary diagnoses, and now I have just that much more empathy.
Also, I now know that I can write a DPC News Blog article with one eye, and that having half the vision apparently doesn’t remove half of the words I write. Sorry.
Next-to-last thing: I have discovered the creepiest thing to do when you have central scotoma. Dear reader, I hope you never get it, but if you do, you gotta try this: Close your “good” eye and look into a mirror, focusing on your bad eye. Your open eye disappears to itself, the eye looking at it. You see your face, but no open eye in the middle of it. My brain freaks out because my eye is simultaneously telling my brain that it exists (I have vision) but when the brain processes the image, there’s no eye there that should be what is sending it the data. My [very simple] brain: “Wait, if the left eye doesn’t exist, how am I seeing with it?”
Every doctor wants an eponymous condition to carry his or her name into the distant future and create some egocentric medical heritage. …And I’m no different! This one is mine. I’m calling it Lassey’s Scotoma Paradox. I googled this phenomenon. After about 15 seconds of solid research, I can’t find anything in the top 10 google result summaries. I’d say we can call this research thoroughly completed, so please go ahead and start teaching your medical students about Lassey’s Scotoma Paradox.
Last thing (I promise): The punch line to the true story about all the medical students taking a dozen teaspoons of random peds drugs has yet to be written. But it’s gonna kill.





