RVUmissing Being In The System?
Why would anyone still be employed? Yes, jumping into Direct Primary Care is NOT easy. It’s simple. There’s a difference. You have tons of resources and peers to lean on, but you will be working hard to fill your practice, and your income will take a hit for a couple of years, at least. That being said, look at how the wRVU system has screwed doctors. And guess who gets paid the least? Yup, family docs.
You can read about it more here.
Here are some more images to explain as well:
and:
So, when the Death Row Syndrome doctors start mouthing off about your journey into Direct Primary Care, show them these images and facts and ask:
- RVUgetting screwed?
- RVUhappy?
- RVUburned out?
- RVUan administrator’s bitch?
- RVUdealing with Stockholm Syndrome?
DPC is NOT perfect, but it is so much better than being employed, and it is the only hope left for primary care.
(Remember, National DPC Day is only 3 months out. It’s time to tell the world about Direct Primary Care).






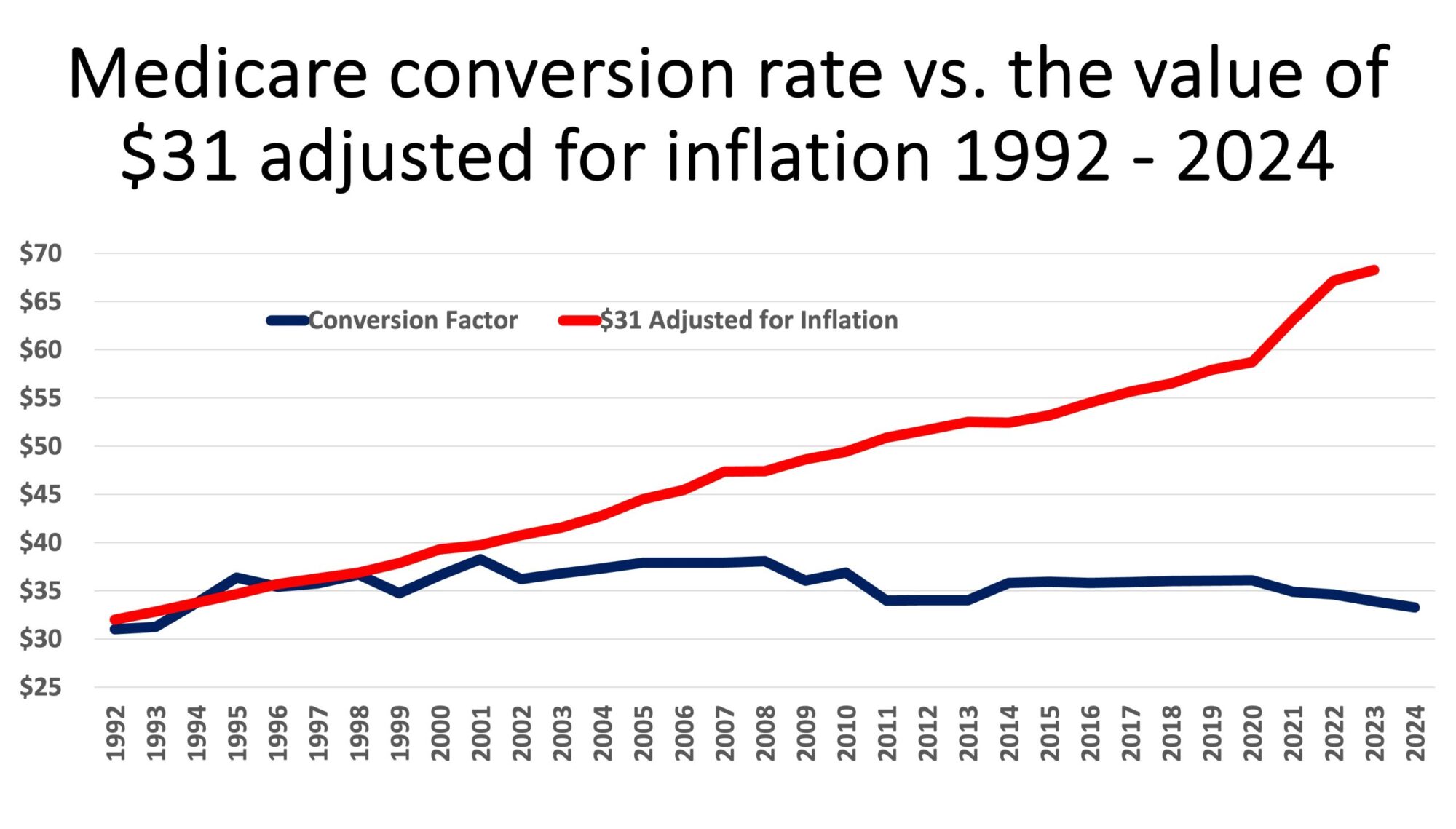
Doug, your information is easy to digest, and I like that it covers the time from when RVU started being a “thing”.
I’ve seen the same information in a different format. A physician in one of the Facebook groups did the following explanation last year. I would assume this person was a proceduralist based on the percentage of overhead and the RVU production, because in FP, overhead in the FFS world is more like 55-70%. This is that doctor’s calculations with a few changes in wording for clarification. Very eye-opening and depressing!
Start with a few baseline ASSUMPTIONS:
1. 1998 physician practice expense = 35% of gross revenue (start with this for illustrative purposes )
2. From 1998 to 2024, typical increase in operating expense (overhead) for physician roughly mirrors the inflation rate of 192.68% (probably a bit worse post-Covid pandemic, but to be conservative assume inflation rate only). **The key is that wages for support staff aren’t controlled by the CMS.**
3. RVU/yr production rate for the physician assumed stable year over year (let’s pick a rate of 15,000 RVU/yr for this)
4. No significant change in RVU per same CPT code in 1998 and 2024.
Scenario 1998:
15,000 RVU X $36.69 = $550,350 (gross)
1998 Expenses = 35% X $550,350 = $192,623
1998 Net Income = $550,350 – $192,623 = $327,757 (this is in “1998 dollars”)
Scenario 2024:
15,000 RVU X $32.74 = $491,100 (gross)
2024 Expenses = 1998 Expense X cumulative inflation = $192,623 X 192.68% = $371,146 (this is a HUGE impact)
2024 Net Income = $491,100 – $371,146 = $119,954 (this is in “2024 dollars”)
Comparing the two scenarios:
1998 net income converted to 2024 dollars:
$327,757 x 192.68% = $689,289
So we see the net effect of inflation and price controls for our payment, but not for our expenses, results in a massive effective income reduction:
$689,289 vs $119,954 — or in other words, effectively we are making +/-18 % of what we made in 1998!!
THE BOTTOM LINE:
1.) CMS’s oppressive price control in the presence of aggressive inflation has degraded real physician income by
+/-80% over the past 25 years.
2.) Although this example uses the CMS (Medicare) $/RVU Conversion Factor, and therefore may not represent your payer mix, realize that this effect has been even more pronounced when you consider that managed care reimbursement has declined relative to CMS rates over time.
So when people say we are overpaid, ask them if they would keep working in the same job if there was, effectively, an 80% pay cut over 25 years.
I thought this guy did a good job of breaking it all down. My 2 cents is below:
10,000 RVUs = 46 RVUs/day for 48 weeks of work. A typical FP visit might generate 1.97 RVUs (appointment, labs, imaging), so doing the math for 48 weeks with 4.5 days of seeing patients (you get 0.5 days for “administrative time AKA prior authorizations”) means seeing 23.5 patients each day (20.4 minutes per patient for everything around the visit, washing your hands, walking down the hall, reviewing the previous note, documenting the current visit, refilling prescriptions, answering questions, and holding the patient’s hand or looking them in the eye). This shows how patients are getting shorted by the current FFS payment model, too!
Wow. Amazing. Thanks for the input!!!